

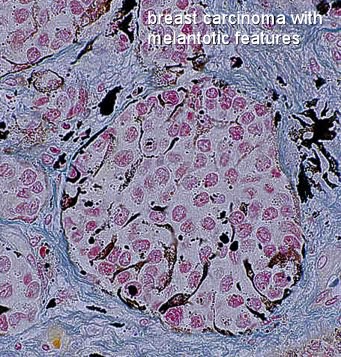
Breast Carcinoma with Melanotic Features
Sometimes breast cancer tumors are found to contain elements of melanocytes within them. This is somewhat unusual because melanocytes are cells found primarily in the skin, and are responsible for the production of the 'dark pigment' melanin (the darker skin color from a 'tan'). When they are found within the same lesion as carcinoma cells (carcinoma is derived from epithelial cells), the tumor might be referred to as 'heterogenous' breast cancer. So, essentially a breast carcinoma with melanotic features is a combination of ductal carcinoma and melanoma.
Heterogenous breast malignancies are very rare, and there is always some interpretation involved as to whether or not the heterogenous (foreign or not typically 'local') elements were part of the breast cancer to begin with (primary), or whether they arrived at the site due to metastasis from a cancer somewhere else. Another possibility is that the presence of melanotic features within breast carcinoma (evidence of melanocytes) indicates that the breast cancer is highly aggressive and has begun to metastize. That was the working hypothesis among breast cancer specialists until fairly recently. New evidence now suggests that melanocytes are actually native to certain kinds of malignant breast carcinoma cells, and do not indicate anything out of the ordinary or 'extra-aggressiveness' of the cancer. In fact, melanocytic elements are now generally thought to be a completely benign and incidental feature of the primary breast carcinoma.
What is 'melanoma'?
Melanoma is a malignant tumor of melanocytes, so essentially a melanoma is a skin cancer tumor. Melanocytes typically comprise between 5% to 10% of the cells in the basal layer of the epidermis, and there are usually between 1000 and 2000 melanocytes per square millimeter of skin. In addition to the skin, melanocytes are are also found in the bowel and the eye. Melanoma is actually one of the less common types of skin cancer, but causes the majority of skin cancer related deaths.(about 75%). One might occassionaly see the term 'nevi' or nevus, ('nevi' is plural), and these refer to 'moles'. A malignant melanoma is typically something which evolves from one of these nevi. Now, it is quite common to develop nevi on the skin of the breast, and some breast nevi cells have been known to have quite atypical features. However, atpyical features of breast nevi have not been shown to correspond to any suspicious biolical behavior and pose no increased risk for melanoma on the breast.
Malignant skin melanomas frequently mestastize to the breast, but a primary breast carcinoma with melanotic features is something completely different.
An important distinction must be made between primary breast carcinoma with melanotic features (the main subject of this page) and breast cancers which develop as a result of metastasis from a primary cancer somewhere else. It is estimated that between 2.7-5.1 % of breast malignancies are due to metastasis, and almost 80% of metastatic breast cancers are from skin cancers. The most likely cancers to metastize to the breast are malignant melanoma, and lung cancer.
Metastastic tumors are slightly more likely in younger women
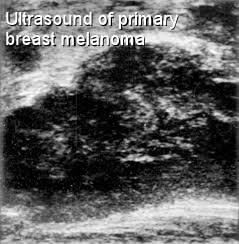
A metastatic breast tumor will usually appear as a painless, solitary, well circumscribed mass in a breast regions rich in glandular tissue. Most of the time, metastatic breast tumors will occur in the upper outer quadrant, which has the most abundtant glandular tissue and also the best blood supply. Younger women are a little bit more likely to develop a metastatic breast cancer tumor because they have increased vascularity compared to older women. A metastatic breast tumor will tend to appear mammographically as a discrete round shadow without spiculation, quite similar in appearance to cinrcumscribed primary breast caricnomas such as papillary and mucinous breast carcinoma. Unforunately, with a metastitic breast carcinoma, most patients do succumb to the illness within one year, with an average survival time of about 11 months.
There are rare instance of malignant melanoma primary to the breast
Malignant skin melanomas characteristically disseminate widely, and metastize to the breast only infrequently (about 3%-5% of the time.) A primary melanoma of the breast is even rarer, but they can arise in the in the glandular tissue of the breast. Sometimes one may find a primary malignant melanoma of the breast arising in the skin of the breast, but without actually developing a cutaneous lesion.
Cause of melanocytic proliferation in breast tumors a matter of speculation only
No one knows exactly why melanotic pigmentation sometimes occurs within breast carcinomas. Generally, melanocytic colonization and pigmentation in breast tumors occurs if the dermal-epidermal junction is involved by the tumor. ( The breast cancer tumor is developing right at the 'edge' of the skin). Perhaps the melanocytes 'migrate' into the breast tumor from the skin. Other theories suggest that the increased proliferation of melanycytes characteristic of breast carcinoma with melanotic features is actually somehow induced by elements already present within the tumor itself.
Melanocyte Growth Factor (MeGF) in breast cancer cells might stimulate the proliferation of melanocytes in breast tumors
Breast cancer cells have sometimes been known to present with transforming growth factors and epidermal growth factor receptors. It is believed that these factors are capable of inducing the proliferation of both normal and neoplastic cells in breast carcinomas. In recent lab experiments, melanocytes have also been shown to proliferate when exposed to an enriched culture medium containing melanocyte growth factor (MeGF, a type of hormone). So, it is hypothesized that it might be the presence of tranforming growth factor in breast cancer cells which would stimulate the growth and heterogenous presence of melanotic features in some breast carcinomas.
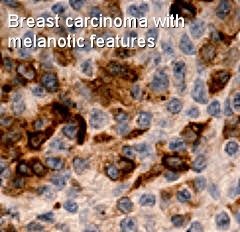
Melanocytic elements within breast carcinoma are observed microscopically, through specific stains.
Microscopically, breast cancer tumors with melanotic features might show abundant deposits of melanin pigment in macrophages and groups of melanocytes among the breast cancer cells. Pigmentation is usually only observed microscopically, but occassionally breast cancer melanosis may be observed clinically. In that situation, one must be careful not to assume that the lesion is a clinically malignant melanoma . Different elements of heterogenous breast cancers such as breast carcinoma with melanotic features will test positive for different stains. The 'carcinoma' element in breast carcinoma with melanotic features might typically test positive for epithelial membrane antigen and CA19-9, while the melanoma component might test positive for for HMB45 and vimentin, and other stains.
New research suggests that melanocytic elements of breast carcinomas might even evolve from genetic alterations of the same clone cells.
Among recent genetic discoveries in the area of breast cancer is the realization that breast cancer cells are not bound by the same 'programmed' cell differentiation course as is the case for normal cells. That might seem to be an obvious conclusion, but, it has been traditionally and somewhat logically believed that if malignant breast cancer cells derive from either mature or immature epithelial cells, then all neoplastic cancer cells which develop would still be within the epithelial cell line. If a non-epithelial cancer cell develops at the same site, it was assumed that it must have migrated to the area from somewhere else, or was perhaps growing adjacent all along. New evidence, however, suggests that some breast cancer cells are not bound to follow the same cell-line, but may in fact differentiate in different cell lines, for example, as melanocytes. This might be a reasonable explanation for a heterogenous breast tumor such as breast cancer with melanotic features. Furthermore, if this is in fact the case, it presents a significant realization that melanocytic elements within breast carcinomas are no more aggressive and worrysome than breast carcinomas without melanocytic features. (Since they are native to the site and have not metastized to the area, the cancer 'staging' is reduced somewhat from the traditional view of heterogenous breast carcinomas with melanoma.)
MDA-MD-435 breast cancer cells prove melanocytic differentiation of primary breast cancer cells is possible, even common.
Recent reports in the area of breast cancer genetics have demonstrated a a wide spectrum of expression of melanocyte-related genes within histologically confirmed breast cancer tumors. In fact, it would appear that aberrant co-expression of multi-lineage markers is actually quite common in breast cancer. By analyzing tumor cells for certain 'molecular signatures' via gene-expression-profiling, one can determine the tissue origin of a given breast cancer cell line. The same genetic alterations with loss of heterozygosity has been noted in both the melanoma and invasive-ductal elements of breast tumors, suggesting that they might have arisen from the same clone-source via multiple genetic alterations during the early stages of breast cancer development (ductal carcinoma in situ).
MDA-MD-435 was discovered in 1976
MDA-MB-435, which is a member of the NCI-DTP panel of 60 human tumor cell lines, has been used for many years as a model of metastatic human breast cancer. (It was discovered in 1976). It has now been shown that the pattern of gene expression for MDA-MB-435 more closely resembled that of melanoma cell lines than traditional breast carcinoma lines. Through analysis, MDA-MB-435 cells have been shown to express melanocyte proteins tyrosinase and melan-A, and RXRG, TYR, ACP5, and DCP, and all of these genes are commonly derived from a melanoma cell line. It has been concluded that the presence of this genetic profile within a common breast cancer cell could not be the result of metastasis, but is actually the product of cell differentiation native to the primary breast cancer. Follow-up studies about the potnetial genetic origins of cancer cells in heterogenous breast cancer tumors have reinforced the notion of abherrant genetic mutation into other cell lines.
References
- Bendic A, Bozic M, Durdov MG. Metaplastic breast carcinoma with melanocytic differentiation. Pathol Int. 2009 Sep;59(9):676-80.
- Nobukawa B, Fujii H, Hirai S, Kumasaka T, Shimizu H, Matsumoto T, Suda K, Futagawa S. Breast carcinoma diverging to aberrant melanocytic differentiation: a case report with histopathologic and loss of heterozygosity analyses. Am J Surg Pathol. 1999 Oct;23(10):1280-7.
- Coley, WB., Hoguet, JP. Melanotic cancer, with a report of 91 cases. Ann Surg. 1916 August; 64(2): 206–241.
- Azzopardi JG, Eusebi V. Melanocyte colonization and pigmentation of breast carcinoma. Histopathology 1977; 1 :2 1-30.
- Nickell KA, Halper J, Moses HL. Transforming growth factors in solid human malignant neoplasms. Cancer Res 1983; 43:1966- 1971.
- Sainsburg JRC, Sherbet GV, Farndon JR, Hams AL. Epidermal-growth-factor receptors and oestrogen receptors in human breast
cancer. Lancet 1985; 1:364-366. - Marco, V., Autonell, J., Cirera, L., Gay, M., Breast Cancer Melanosis in a Postmastectomy Scar. Cancer, Volume 62, Issue 1 p 206-209
- Gadkari R, Pangarkar MA, Lele VR, Bobhate SK, Kher AV. Florid melanocytic colonization in a metastasis of breast carcinoma. A case report. Acta Cytol. 1997 Jul-Aug;41(4 Suppl):1353-5.
- Montel, V., Suzuki, M., Galloy, C., Mose, E. Tarin, D., Expression of melanocyte-related genes in human breast cancer and its implications. Differentiation Volume 78, Issue 5, December 2009, Pages 283-291
- Greene MH. (1998). "The genetics of hereditary melanoma and nevi". Cancer 86 (11): 2464–2477.
- Rongioletti F, Urso C, Batolo D, Chimenti S, Fanti PA, Filotico R, Gianotti R, Innocenzi D, Lentini M, Tomasini C, Pippione M, Rebora A. Melanocytic nevi of the breast: a histologic case-control study. J Cutan Pathol. 2004 Feb;31(2):137-40.
- Howlett AR, Petersen OW, Steeg PS, Bissell MJ (1994) A novel function for the nm23-1 gene: overexpression in human breast carcinoma cells leads to the formation of basement membrane and growth arrest. J Natl Cancer Inst 86: 1838–44.
- Sellappan S, Grijalva R, Zhou X, Yang W, Bar Eli M, et al. (2004) Lineage infidelity of MDA-MB-435 cells: expression of melanocyte proteins in a breast cancer cell line. Cancer Res 64: 3479–85.
- Hollestelle A, Nagel JH, Smid M, Lam S, Elstrodt F, et al. (2009) Distinct gene mutation profiles among luminal-type and basal-type breast cancer cell lines. Breast Cancer Res Treat. (May 2010) Volume 121, Number 1 , p. 53-64
- Neve RM, Chin K, Fridlyand J, Yeh J, Baehner FL, et al. (2006) A collection of breast cancer cell lines for the study of functionally distinct cancer subtypes. Cancer Cell 10: 515–27.
- Ellison G, Klinowska T, Westwood RF, Docter E, French T, et al. (2002) Further evidence to support the melanocytic origin of MDA-MB-435. Mol Pathol 55: 294–9.
- Cailleau R, Olive M, Cruciger QV (1978) Long-term human breast carcinoma cell lines of metastatic origin: preliminary characterization. In Vitro 14: 911–5.
- Lacroix, M., MDA-MB-435 cells are from melanoma, not from breast cancer. Cancer Chemotherapy and Pharmacology. (Feb. 2009) Volume 63, Number 3,p. 567
- McGovern VJ, ed. Melanoma. Histological Diagnosis and Prognosis. New York: Raven Press, 1983: 78.
- Kim, TY., Chae, MK.,Kim, HH, Kim, SY.,Baek, MJ., Lee, MS., Kim, CH., Kim, EH., Lee, MK., Cho, MS., Song, OPA case of Malignant Melanoma Presenting as a Breast Mass. Journal of Korean Breast Cancer Society 2003; 6:35-38
- Vergier, B., Trojani, M., de Mascare, I., Coindre, JM., Le Treut, A. Metastasis to the breast: differential diagnosis from primary breast carcinoma. J surg Oncol 1991; 48: 112-116.
- Toombs, BD, Kalisher, L, Metastatic disease to the breast: cl.inical, pathologic, and radiographic features. Am J Roentgenol 1977;129:673-6.
Back to Types of Lesions list.
End of page Navigation links: Breast Cancer home or Back to top
Copyright © 1999 - present. Steven B. Halls, MD . 1-780-608-9141 . [email protected]